Highlights
Birth rates in America, and around much of the world, are lower than what women say they want. This is the incontrovertible conclusion from looking at the data we have on birth rates and women’s fertility preferences. But it’s a strange finding: it seems like if people wanted more kids, they could have them. What explains this durable gap in fertility between what is achieved and what is desired?
C-Section Births Reduce Future Birth Rates
One surprising answer that may account for a portion of the gap is the frequency of Caesarean deliveries. While it may seem strange to attribute society-wide changes in birth rates to a specific method of delivery, it turns out to be eminently plausible. Academic researchers have shown for decades that having a C-section reduces the odds of having future children. The only question was why and how. Studies in Denmark suggest this effect was driven by women getting non-emergency C-sections. Other studies suggest C-sections actually might alter the biological capacity to conceive.
But aside from these channels, it is also fairly uniformly acknowledged among doctors that having multiple C-sections can carry significant health risks for women and infants. C-sections are a vital tool for safely delivering many babies, but women who’ve had two to four C-sections are usually advised to avoid becoming pregnant again. The more common C-sections are in a society, the larger the share of women who face extra health risks if they have a third, fourth, or fifth child. In other words, we would expect that a higher prevalence of C-sections would result in a lower prevalence of higher-parity children.
Health Risks from Higher-Parity C-Sections Lower Fertility
Interestingly enough, the international Demographic and Health Surveys supported by the U.S. government ask women about delivery methods, and thus we can get extensive data on C-section rates around the world. In a series of panel regressions with fixed effects for country and year, using a panel composed of mostly developing countries due to data limitations, I find that, controlling for aggregate fertility rates, a higher C-section prevalence suggests a larger share of women will stop at one or two births, and a smaller share will end up having three or more births. Crucially, by controlling for the total fertility rate, I’m not picking up changes in how many kids the average woman has, and I’m implicitly controlling for a country’s level of economic modernization. This model, very simply, tells us: is a higher prevalence of C-sections actually associated with fewer women achieving higher numbers of births?
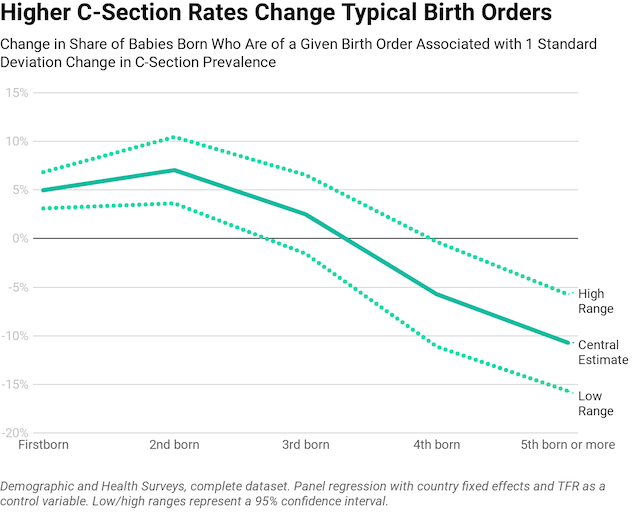
The answer is a resounding yes. With more C-sections in a given society, fewer women will have higher-parity births. For a society to have a given total fertility rate with a higher C-section rate, they would need to have fewer women end up childless, i.e. they’d achieve their birth rate by having more women become mothers at all, while fewer women would have 3 or more kids. Basically, this model tells us that having more C-sections really is associated with fewer women having a larger number of births.
But I controlled for a country’s total fertility rate in that model, which was a very strict test to see if there was any reason to think C-sections matter. If C-sections were not associated with differences in parity-achievement, there’d be no reason to investigate further. But since C-section prevalence actually does associate with birth parities, there is a reason to look deeper.
A second panel model can be estimated with variables controlling for the share of women who have been sterilized, the share of women using other modern forms of contraception, child mortality, wives’ control of their own health decisions, agriculture’s role in the economy, and, of course, the prevalence of C-sections. I also include variables for the coincidence of C-section prevalence and female sterilization, as well as C-section prevalence and wives’ control of their own health decisions. Before sharing my results, I should explain these last two.
There is some research that suggests that in countries with poor access to contraceptives, or where women have imperfect control of their own health and fertility decisions, women may seek out sterilization at greater rates. This is a “last resort” method of fertility control. This line of reasoning suggests that C-sections are often preferred in these countries because female sterilization procedures can be rolled into the C-section procedure. Thus, it could be the case that C-sections reduce fertility, but only because they are actually measuring the prevalence of “two-in-one” surgical procedures: delivery a baby, then sterilize the mom. Including interactions of C-sections with wives’ health autonomy and sterilization helps us explore this possibility.
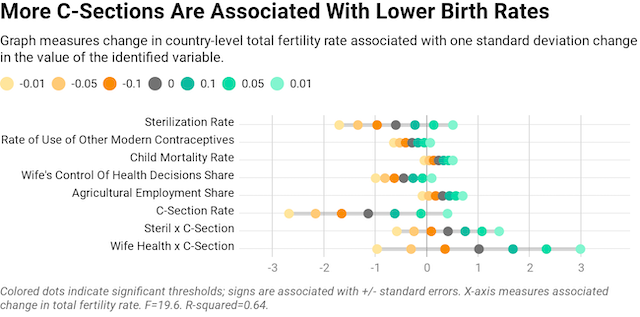
C-sections turn out to be a large and statistically significant predictor of fertility rates, even with numerous controls. The estimated effect size for one standard deviation of change in C-section prevalence is larger than for any other single variable, and it has a similar level of statistical significance as the use of contraceptives, wives’ control of their own health, or a country’s child mortality rate. The C-section estimate is less precise than some of those other, more conventional factors, but still significant.
Meanwhile, our interaction effects are not statistically significant at conventional levels. And even if they were, they would not confirm the story that C-sections reduce fertility via the channel of sterilization: the joint incidence of C-sections and sterilization actually predicts higher fertility. The same goes for the interaction of wives’ control of their own health decisions and C-sections.
In other words, C-sections reduce fertility, and not primarily through sterilization. They reduce it some other way. My suggestion would be that they probably reduce fertility through the channel already identified: reducing higher parity births as women avoid the greater health risks associated with repeated C-sections. This theory can be tested by swapping out our independent variable: instead of predicting the total fertility rate, we want to predict the share of women who will reach a given parity of childbirth. To simplify this exercise for readers, I will show the final outputs of the regressions for each parity of birth, represented as the percent change in the share of women who reach a given childbearing parity associated with one standard deviation in C-section prevalence.
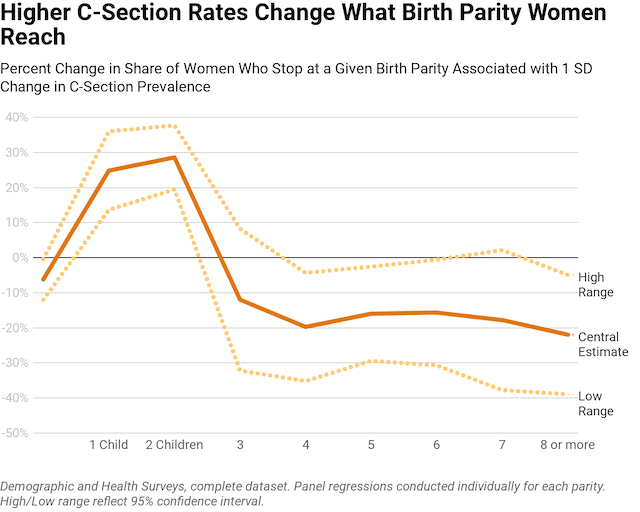
As can be seen, higher rates of C-sections are associated with more women stopping at just 1 or 2 children, and fewer women having 3 or more births. This is, again, precisely in line with what we would expect if in fact C-sections cause women to avoid higher-parity births.
C-Sections Are Becoming Increasingly Common
Why does any of this matter? Why should we be concerned about C-sections?
C-sections are becoming increasingly common around the world, despite no corresponding increase in the need for emergency deliveries. The rise in medically unnecessary C-sections is so alarming, dangerous to moms, and perplexing that the prominent medical journal, The Lancet ran an entire series of articles, cataloging the abuse of C-sections for discretionary purposes. The World Health Organization recently published guidance, urging countries to reconsider excessive C-sections, noting that C-section rates over 10% are not associated with any improvement in women’s health or child mortality. This is striking, because, globally, C-sections accounted for just 6% of global births in 1990, while they account for 21% today.
Medical practitioners and scientific experts have referred to this rise of unnecessary C-sections as an “ epidemic.” The blistering pace of increase in a medically unjustifiable surgery that can permanently impact a woman’s health, wellbeing, and fertility is deeply concerning.
While the jury is still out on the exact causes of this increase, at least some of it is cultural. For example, many Asian countries like Thailand have unusually high C-section rates. One reason why is because the local religions have strong beliefs about lucky and unlucky times to be born. There are certain months, days, and years considered more auspicious for a birth. Thus, there are strong cultural incentives for birth scheduling and, thus, for C-sections, a common method of achieving a planned birth. Parents in Thailand report picking C-section dates to get lucky birthdays, sometimes even down to the minute of delivery. Around the Chinese New Year, parents often try to schedule births to land on one side or the other of auspicious dates, to get their child a preferred zodiac association.
But cultural preferences don’t only drive excess C-sections on foreign shores. Using U.S. daily birth data from 1969 to 2014, it’s possible to estimate the extent to which American parents systematically avoid certain days. Basically, by assessing the extent to which the number of births on a given day varies from the average number of births within 2 weeks before and after, we can see to what extent American parents are scheduling births: avoiding certain days and trying to have babies on other days. This metric of birth planning turns out to correlate closely in recent years with the frequency of C-sections.
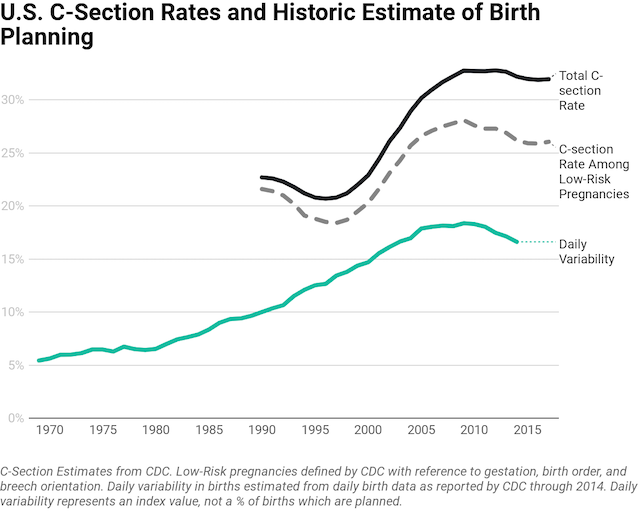
American cultural preferences drive C-sections too! American families strongly avoid having babies on weekends and holidays, as I’ve shown in prior research. The increasing American prevalence of planned births, micromanaged fertility, andpreferences for specific birthdays, drove a sharp rise in planned births over the last two decades.
But after the recession, birth planning tailed off a bit, as did C-sections. It’s unclear why: it may have been due to changed medical guidelines for C-sections, changed cultural preferences, decreased economic circumstances, or any number of other factors. There is no data on daily births more recently than in 2014. But the key point is that when we think about cultural norms driving C-sections, we shouldn’t just imagine idiosyncratic norms in other countries—there are norms and values within American society causing the same trend.
Conclusion
C-sections create additional medical risks for women who want to have more children. As a result, a higher rate of C-sections predicts a lower overall fertility rate, driven by greatly reduced births at higher birth parities. Thus, it’s reasonable to think that a higher prevalence of C-sections may lower birth rates, especially since the medical literature on C-sections strongly supports the idea that, at the individual level, C-sections reduce subsequent birth rates among impacted women.
My exploration of data from the Demographic and Health Survey database confirms that, at least in developing countries, higher C-section rates are strongly associated with reduced fertility, specifically through the channel of reduced high-parity births, and not driven by greater reliance on sterilization. In a supplementary analysis not presented in detail here, I also expanded the DHS dataset with indicators of births and C-sections in a sample of developed countries and found that the same relationships held, although differences in data reporting between the two datasets reduced the significance of all variables somewhat.
For societies that want to help women achieve their desired birth rates and avoid excessive health risks to women, one solution could be to discourage medically unnecessary C-section deliveries. While this reduces the choices available to women for their own delivery, there are versions of the policy that are consistent with pluralism and liberal values. Doctors could be encouraged to educate women about the risks associated with elective C-sections more directly. Regulations vary across countries, but doctors could be given more legal and informal rights to decline to provide medically unnecessary C-sections. As more doctors exercise a right to opt out of elective C-sections, the total prevalence may decline.
But one way or another, it is important to understand that a considerable amount of fertility decline is not only about improving women’s wellbeing and economic changes. To some extent, fertility decline is also being driven by cultural preferences for medically unnecessary procedures that reduce future fertility rates and endanger many moms.
Lyman Stone is a Research Fellow at the Institute for Family Studies, and an Adjunct Fellow at the American Enterprise Institute.